Myocardial Infarction, the irreversible destruction of the heart muscle, can be due to many pathophysiological mechanisms. Today we will talk about different types of Myocardial Infarction and their symptoms.
Myocardial distress manifests by an elevation of cardiac troponin I or T. These are essential proteins of the contractile system of the cardiomyocyte. The increase in their blood level specifically reflects the necrosis of the cell. And maybe accompanied by clinical symptoms inconsistently. You can acute the suffering – in the event of an initial rise followed by a fall in troponin. Or chronic, this marker is remaining stable, as in severe chronic renal failure or structural heart disease. However, myocardial distress is always a sign of seriousness. Regardless of the etiology, it does not necessarily indicate a myocardial infarction (MI).
We speak of IDM if the suffering is of ischemic origin. That is to say, linked to a mismatch between the myocardial need for oxygen. And the blood supply provided by the coronaries. Classic manifestation, whatever the underlying cause, chest pain is retrosternal (burning, weight, or tightness), bar. Radiating to one or both arms or the lower angles of the jaw. The ECG can then show changes in the ST segment, elevation or depression, flattening. Or even negotiation of the T wave. It is sometimes normal.
5 Types of myocardial Infarction
In collaboration with the WHO, the European and North American Cardiovascular Societies distinguish 5 types of infarctions. Each is linked to a specific mechanism.
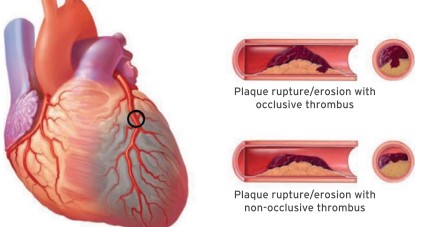
IDM type 1: classic!
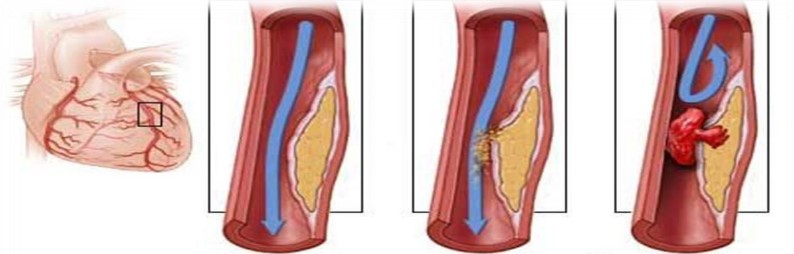
It linked to the occurrence of a coronary thrombus by rupture or cracking of an atherosclerotic plaque.
Complete obstruction induces acute coronary syndrome (ACS) with ST-segment elevation (ST +). 2 This therapeutic emergency requires immediate transfer to a structure. A coronary angiography technical platform for revascularization by angioplasty (or fibrinolysis in the absence of immediately available imaging). It would help if you also urgently administered an anticoagulant (enoxaparin or unfractionated heparin). And 2 antiplatelet agents (aspirin and P2Y12 receptor inhibitor, prasugrel, or ticagrelor) promote coronary disobstruction.
A partially obstructive thrombus or causing a distal coronary embolus causes ACS without ST elevation (ST-) but with troponin elevation. Coronary angiography requires within 24 hours. Or even immediately in case of chest pain refractory to the administration of nitro derivative. Anticoagulant and antiplatelet monotherapy is urgent. While it recommends postponing the administration of anti-P2Y12 until angioplasty to reduce the risk of bleeding. 3, 4
In most cases, so-called active stent implants, that is to say, cover with an agent preventing coronary restenosis. The risk of thrombosis from this device has decreased considerably with the advent of active stents and is 2 to 3 times lower than the recurrence rate (rupture of plaque) elsewhere. Bare stents are no longer recommended due to their high likelihood of restenosis and serious cardiovascular event.
You must maintain dual antiplatelet therapy for at least 1 year. In the event of a low risk of bleeding (young patient, not taking an oral anticoagulant). And significant ischemic risk (recurrent coronary artery disease, diabetes, numerous stents) can prolong it beyond 1 year. For patients on anticoagulants, especially direct oral anticoagulants ([DOA], for AF, mechanical valve, MTEV), it is now possible to stop aspirin after a short period, generally <15 days, and to maintain the anti- P2Y12 in addition to DOA. 5
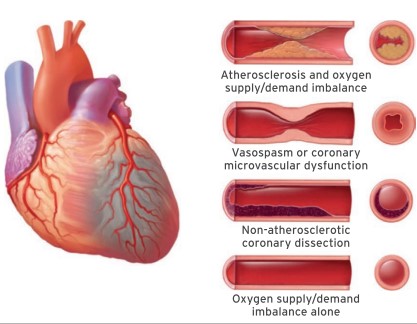
IDM type 2: no thrombus
The decrease in coronary perfusion is due to a local (spasm, spontaneous dissection, or coronary embolus) or systemic cause (hypotension or shock, severe bradycardia, respiratory failure, or severe anemia) or to increased oxygen requirements (sustained arrhythmia or severe hypertension). We speak of a “functional” infarction, which is more common in the case of underlying atheromatous coronary disease. This Infarction may be accompanied by clinical and electrical manifestations of ACS, including ACS ST (+). A more or less urgent coronary angiography may be necessary, depending on the context, to eliminate an acute thrombus or to manage a coronary atheroma revealed on this occasion. Urgency: identify and treat the cause of the mismatch between need and O 2 supply (correction of hypotension or hypertension, hypoxia, anemia, etc.).
Supported
In the intensive care cardiology unit (ICU), coronary circulation assess (coronary angiography). And the extent of muscle damage (cardiac ultrasound and MRI). In type 2 IDMs, correcting the cause of ischemic suffering (hypoxia, anemia, etc.) is crucial. For type 1: urgent reperfusion associated with the antithrombotics as mentioned earlier. In addition, you require aggressive secondary prevention due to the underlying atherothrombosis. It includes a high-dose statin (atorvastatin 80 mg/day with a target LDL of 0.55 g / L or even 0.4 if recurrence), with Ezetrol from the start of hospital treatment. The severity and extent of the atheroma may motivate the cardiologist to prescribe an antiPCSK9: alirocumab, available post-ACS depending on the residual LDL and the severity of the coronary damage (Multitronic patients) and other localizations (AOMI in particular).
Recently, low-dose colchicine has shown interest: in synergy with lipid-lowering drugs, it stabilizes plaques, reducing recurrence. Finally, to prevent complications (heart failure in the event of significant sequelae), drugs inhibit the renin-angiotensin system (IEC, ARB2, and anti-aldosterone), which fight against fibrosis and cardiac remodeling.
Rhythm disturbances prevent by a beta-blocker, the usefulness of which is still topical in the hospital phase and at least during the first 6 months.
Beyond that, it is debatable in the absence of recurrence, significant sequelae of heart failure. It assesses by the ABYSS study conducted by our ACTION heart group with the support of a national PHRC.
FRAME
Other heart attacks: interest in comparing curative strategies.
Type 3 MI includes deaths that appear to be due to a coronary cause, without the possibility of dosing troponin or doing an ECG before the fatal outcome.
Type 4 designates infarcts secondary to percutaneous coronary intervention (4a within 48 hours after the procedure; 4b and 4c in the event of thrombosis or stent restenosis, respectively, regardless of the delay).
Type 5 MDI defines ischemic myocardial distress occurring within 48 hours of coronary artery bypass grafting.
People who have had a myocardial infarction (MI or “heart attack”) require urgent care. Once the heart attack is treated, patients will receive long-term care to prevent a new heart attack and avoid cardiovascular complications after a heart attack. This post-infarction care is based on several therapeutic modalities: drugs, cardiovascular rehabilitation, lifestyle measures, and, sometimes, surgery.
What are Myocardial Infarction and their types?
The Myocardial Infarction, or heart attack, destroys part of the heart muscle when oxygen is no longer supplied. What happens when an artery that irrigates becomes blocked or suddenly decreases in diameter? That happens, for example, when a fragment of fatty plaque breaks off from the inner wall of a blood vessel and clogs an artery in the heart. A blood clot then forms, which causes part of the heart to suffocate.
The oxygen-deprived myocardial cells die, and the affected area, more or less extensive, can no longer contract properly. As the death of muscle cells occurs within approximately four hours of the onset of the Infarction, a myocardial infarction is a medical emergency that ALWAYS requires calling the EMS (15 or 112).
What are the symptoms of Myocardial Infraction?
The symptoms of Infarction are chest pain that lasts more than 20 to 30 minutes. It radiates behind the breastbone, in the back, shoulders, jaw, and left arm. Other symptoms are possible: anxiety, sweating, dizziness, shortness of breath, for example. These pains can be localized in the stomach or belly in women, which is rarer in men. They can be accompanied by nausea, vomiting, or sudden severe fatigue.
Certain infarcts can often go unnoticed and are discovered during an electrocardiogram performed during a health check-up.
FAQ on types of Myocardial Infarction
Do I have a new myocardial infarction?
During a second heart attack, the symptoms may be different. Therefore, you must be vigilant about what you feel and react as quickly as possible, regardless of the intensity and duration of the pain. The patient or his entourage should never hesitate to call the Samu (15 or 112). You should try to stay calm, do not drive, and if possible, take aspirin and your vasodilator medicine if your doctor has prescribed one.
What is the prognosis of a Myocardial Infarction?
In the USA, each year, approximately 100,000 people are victims of myocardial Infarction. It is a potentially serious disease, but major progress has been made in managing heart attack: today, 96% of people who have a heart attack survive beyond one month, and 89% survive beyond one year.
All patients do not have the same prognosis after a heart attack, depending on their age, their sex, the existence of cardiovascular risk factors (such as tobacco, excess cholesterol, or diabetes, for example), and of course, depending on the severity of the Infarction.
What are the complications of Myocardial Infarction?
The consequences of myocardial Infarction are more or less important depending on the extent of the area of the heart muscle affected and the speed of implementation of emergency treatment. The severity of the damage to the heart muscle is assessed by various medical examinations: electrocardiogram, cardiac ultrasound, coronography, scintigraphy, for example (see box below). In addition, it is possible to measure certain cardiac enzymes in the blood which release during the destruction of cells.
What is a cardiac arrhythmia in an infarct?
The risk of sleeping in the suites of an IM is much higher than those present: a cardiac frequency or reps> 75 bpm. An increase of cardiac frequency at effort <89 bpm. A decrease of cardiac frequency <25 bpm 1 min after a stress test.
Conclusion on types of Myocardial Infarction
Myocardial Infarction happens that a second heart attack announces itself a few days or a few hours in advance: the feeling of malaise, tiredness, nausea, problems of digestion, for example. In this case, it is important to consult your doctor quickly.
The complications of myocardial Infarction are diverse: stroke, chronic heart failure (70% of chronic heart failure are due to a heart attack), recurrences (repeated infarctions), and arteriopathy obliterating of the lower limbs (the arteries of the legs close up). Post-infarction care consists of implementing measures to prevent these complications in a lasting manner.